Two crowns, one balanced smile — Ms. Ammarah's anterior rebuild.
Ms. Ammarah is a 37-year-old patient who walked into our Engineers Town clinic with a single, specific request — to fix the way her two upper front teeth no longer matched each other in a photograph. One of her central incisors had drifted downward into a long, dominant shape; the other had tilted gently inward toward the palate. The asymmetry was not a problem of disease. It was a problem of proportion. This is the full story of how two carefully planned zirconia crowns gave her back the smile line she remembered.
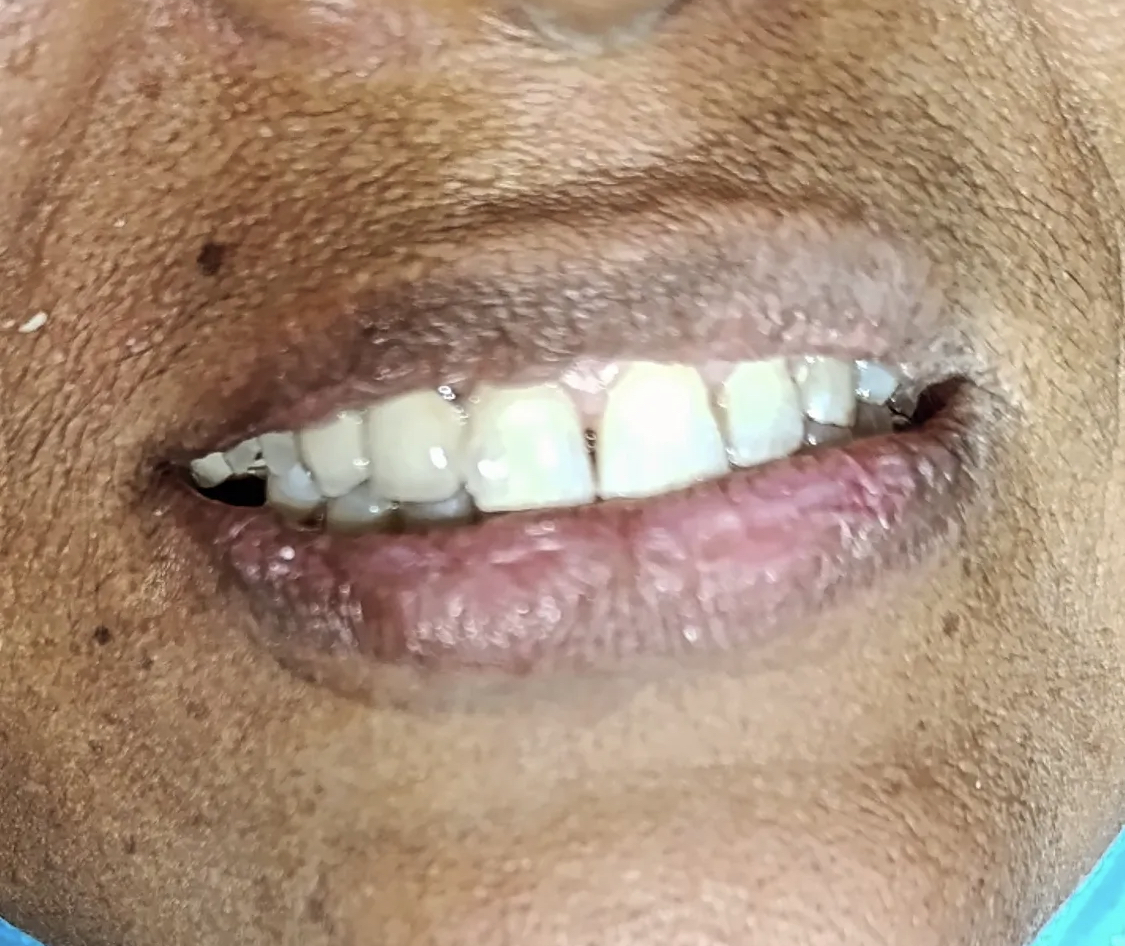
 Before
Before After
AfterOne tooth too long. One tooth tilted back. A smile she no longer recognised.
Most cosmetic crown cases at this clinic are not patients with broken teeth or visible decay. They are patients whose front teeth have drifted — slowly, painlessly, over a decade — out of the line they used to be in. Ms. Ammarah is exactly that kind of case.
Ms. Ammarah came to see us in the early part of last year. She is thirty-seven, a working professional who lives a twenty-minute drive from our clinic, and the kind of patient who arrives at consultation with a clearly worded set of concerns rather than a vague worry. She placed her phone on the desk and pulled up three photographs — one from her own wedding eight years ago, one from a recent family gathering, and one taken in front of her bathroom mirror that morning. In all three, the upper-right central incisor looked noticeably longer than the upper-left one, and the upper-left one looked slightly set back from the lip line.
She did not know any of the dental words for what was happening. She had two words of her own: "lopsided" and "uneven". She had stopped smiling fully in photographs for around two years. She was not in any pain. She had not had a cavity in years. She brushed twice a day, used floss inconsistently, and visited a dentist roughly once a year for cleanings. None of this was a problem of disease. It was a problem of proportion — and that proportion problem had quietly become a confidence problem.
When we sat her in the chair and shone the operating light into her mouth, we saw exactly what she had described. The upper-right central was supra-erupted — that is, it had drifted downward into a space where nothing was holding it back. We measured it carefully against the adjacent lateral incisor and the contralateral central, and the incisal edge sat about one and a half millimetres lower than the symmetric position would have placed it. The upper-left central, in contrast, had tilted palatally — its labial face angled gently backward toward the roof of the mouth. From the front this made the left central look both shorter and narrower than its partner.
We took six standardised intra-oral photographs from the same angles we photograph every patient — a frontal, two laterals, an upper-occlusal, a lower-occlusal, and a close-up of the maxillary anteriors in light retraction. We took two periapical X-rays of both central incisors and a single panoramic radiograph for a wider view. Then we walked her through what we were seeing.
The bone was completely intact. Both teeth tested vital on the cold-stimulus pulp test. No caries. No prior restorations on either incisor. Periodontal probing depths were all under 3 mm. The lateral incisors and canines either side were also healthy, with no rotations and no decay. This was, from a biological standpoint, a textbook healthy mouth — with two teeth that had drifted into a position no orthodontist had ever stabilised.
We laid out three options and we walked through each in plain language. Option one was orthodontics — Invisalign aligners or fixed labial braces, for somewhere between fourteen and eighteen months, to physically push the supra-erupted central back up into the bone and tip the palatally tilted central forward into line, after which both teeth would need a fixed lingual retainer wire bonded behind them for life. Option two was four veneers — minimal-prep on the upper canines, slightly more reduction on the laterals, and fuller-prep porcelain on the two centrals — to mask the asymmetry behind a symmetrical veneer set across all four anteriors. Option three was two zirconia crowns, limited only to the two central incisors, with all proportion correction built into the shape of the crowns themselves.
She listened. She asked sensible questions — how long for each, how expensive each, what could go wrong, what would the worst-case follow-up look like. She took two weeks to think it through with her husband and a sister who works as a pharmacist. She came back on the morning of February the third with her decision: two crowns, only on the centrals, no orthodontics, no veneers on the laterals. Her stated reason was that she did not want to be in any kind of appliance during the year she was scheduled to appear in her brother's wedding photographs, and she preferred the most direct route to a symmetrical front-teeth shape.
We respected that decision, documented her informed-consent signature on the treatment plan she had initialled, and booked her in for the preparation visit. The case began.

Four things — explained in plain English.
For a cosmetic case we always start by telling the patient what is healthy and what is not. The patients who already worry about their smile do not need to also worry about hidden problems they cannot see.
A supra-erupted upper-right central
When Ms. Ammarah closed her teeth together and we held a small mirror up at chair-side, the upper-right central incisor was sitting noticeably lower than its neighbour — about one and a half millimetres below the line of the other front tooth. In dental terms we call this supra-eruption: the tooth had drifted downward into a space that nothing was holding it up against, probably for years. The visual effect was a long, dominant front tooth on one side and a normal-looking tooth on the other, and that single millimetre-and-a-half of asymmetry was doing most of the work of making her uncomfortable in photographs.
A palatally tilted upper-left central
The matching tooth on the left side, in contrast, had drifted gently inward toward the palate. The crown tipped slightly backward, so from the front it looked shorter, narrower, and set back relative to its mirror partner. When we shone a small intra-oral light across the labial surface, the left central caught the highlight at a different angle to the right — a classic sign that two adjacent teeth are in different positions in three-dimensional space, even when they look only "slightly off" to the patient.
A disturbed anterior smile line
Together, the supra-erupted right and the palatally tilted left produced what we describe as a broken smile line — the curve traced by the incisal edges of the upper front teeth no longer flowed smoothly with the lower lip. A balanced smile has the central incisor edges sitting parallel to, and lightly touching, the curve of the wet-dry border of the lower lip. Hers did not. The eye picks up that imbalance immediately, even when the lay observer cannot name what is wrong.
Healthy tooth structure underneath
Almost everything else in the chart was reassuringly normal. The bone level around both centrals was completely intact on radiograph. There was no decay, no caries activity, no soft pulpal symptoms — both teeth tested vital. Periodontal probing depths were under 3 mm at all six points around each tooth. From a biological standpoint, the case was about aesthetics and proportion, not disease.
Four steps. Three visits across two weeks.
Every step was explained before it happened and shown to her in a mirror at the time. She kept the temporary acrylic crowns for two weeks before final cementation, so she could try the new shape on her face in real life — not just in a wax-up.
Consultation, photographs and shade study
Ms. Ammarah came in for a standalone consultation visit before any preparation began. We took six standardised intra-oral photographs, two extra-oral views with her natural smile, and a set of detailed close-ups of both central incisors. With the photographs on the big screen next to her, we walked through her three real options — orthodontics to physically move both teeth back into line, veneers on four anterior units, or two zirconia crowns limited to the two centrals. Each option had a real list of pros and a real list of cons. She decided on the two-crown plan that same afternoon.
Day 1 · ~ 45 minTooth preparation under local anaesthesia
At the second visit we numbed the two upper centrals with a buccal infiltration of 4% articaine. Preparation was conservative — we removed about 1.0 mm of enamel from the labial surface, 1.5 mm from the incisal edge, and a tapered shoulder finish line just at the level of the gum. Both teeth received a digital scan and a temporary acrylic crown shaped slightly closer to the planned final aesthetic, so she could try the new shape on her face for two weeks before signing off the final restorations.
Day 2 · ~ 70 minTry-in and final cementation
The zirconia crowns came back from the dental laboratory at the end of the second week. We tried them in on the prepared teeth before cementation and checked five things in order — the marginal fit at the shoulder, the proximal contacts to the adjacent lateral incisors, the occlusion in centric and protrusive movements, the gum response at the cervical margin, and the way the two crowns photographed against her natural lip. Everything passed first time. They were cemented with a dual-cure resin cement and the excess was removed under magnification.
Day 3 · ~ 50 minPolish, occlusal balance and home care plan
A fine polishing burr smoothed the labial surface to a mirror finish, and a small grain rubber wheel softened the incisal edge so it would not feel sharp when she ran her tongue across it. We checked the bite one more time with articulating paper to make sure no premature contact had developed since the morning. She left with a printed home-care sheet, a written maintenance schedule, and the WhatsApp number to reach us with any question in the first 72 hours.
Day 3 · ~ 15 min During — preparation phaseAfter — final cementation
During — preparation phaseAfter — final cementationSame patient. Same lip. Same lighting.
Drag the divider across the photo to compare. Both photos were taken with the same camera and lighting inside our Lahore clinic — "before" at the consultation, "after" on the day of final cementation.
BeforeAfterWhy zirconia, and why two crowns rather than four veneers.
Patients reasonably ask why we recommend one material over another, and why we restrict treatment to two teeth when many clinics would have proposed four. The honest answer has three parts. None of them are about cost.
Zirconia is stronger than e.max for posterior loads — and now beautiful enough for anteriors
A decade ago, monolithic zirconia was a strong but unaesthetic material — chalky white, low translucency, and obviously different from natural enamel in close inspection. Modern multi-layered zirconia blocks change that. Each block has three to four shade gradients pre-built into the disc, and a translucency tuned to match the optical behaviour of natural enamel from cervical to incisal. The result is a crown with the body strength of zirconia and a layered aesthetic close to traditional porcelain. For a 37-year-old with a normal bite, that combination is durable and aesthetic at once.
Veneers on healthy laterals would have meant cutting teeth that didn't need cutting
The four-veneer plan would have asked us to remove between 0.5 mm and 0.8 mm of natural enamel from the upper laterals and canines — teeth which, in Ms. Ammarah's case, were perfectly proportioned and in good position. The principle of minimal-invasive dentistry is that you only prepare what you need to prepare to solve the actual problem. Her actual problem was on the two centrals. The two-crown plan respects that principle. The laterals and canines remain untouched.
Two crowns over twenty years is a fixable maintenance plan
Crowns do not last forever, and any dentist who tells a patient otherwise is mis-selling them. What zirconia gives us is a realistic 15-to-20-year service life when the gum and bone underneath are well maintained. When the two centrals eventually need replacement — somewhere around 2040 to 2045 if her home care holds — only those two crowns will need re-doing. Four veneers would have meant four units to re-do at the same point, on teeth that were originally healthy. Conservative choices now lower the total cost of dental care over a lifetime.
Five questions we hear at every anterior crown consultation.
These are the worries we heard from Ms. Ammarah, and the worries we hear from most patients who consider anterior crowns. Tap any one to read the long answer.
Will the two crowns look obviously different from my other teeth?+
This is the single most common worry we hear before a two-tooth front crown. The honest answer is: not when the case is planned properly, and almost always when it is not.
The reason a crown can look "fake" is rarely the crown itself — it is a mismatch between the layered shade of the crown and the slightly translucent enamel of the adjacent natural tooth. Zirconia in 2025 is no longer the chalky-white opaque material it was a decade ago. The blocks we use are layered, with three or four shade gradients from cervical to incisal, and a translucency profile tuned to match natural enamel optical behaviour. That means the crown can be made to imitate the way light passes through the body of the tooth and bounces off the incisal edge.
For Ms. Ammarah, we did a chair-side custom shade match against her two adjacent laterals under both daylight and clinic light, and the laboratory came back with two crowns whose shade we then re-checked at try-in before cementation. A second try-in lets us catch any "too white at the incisal" or "too grey at the cervical" issue while the crown can still be sent back. That extra ten minutes is the difference between an invisible result and an obvious one.
Six months after cementation she came in for a routine review and showed us a photograph from her sister's wedding. Her friends could not tell which two teeth were the new ones — even when she pointed and told them.
How long do zirconia crowns last? Will I have to redo them every five years?+
Properly designed monolithic zirconia crowns on healthy abutments routinely last 12 to 20 years in the published literature, and we have several patients at this clinic who are now past the 10-year mark on their original crowns with no marginal breakdown.
The single biggest predictor of crown longevity is not the brand of zirconia or the cement used — it is the health of the gum and bone underneath the crown. If the cervical margin stays plaque-free, the crown will outlast many other things in dentistry. If plaque is allowed to gather at the margin, the gum will inflame, recede, and eventually expose root surface that the crown was never designed to cover.
That is why we ask every crown patient — and we asked Ms. Ammarah specifically — to floss every night around the crown margin, and to come in for a six-month marginal check whether the rest of the mouth needs a clean or not. Twenty years is realistic if those two habits are kept.
Why didn't you recommend braces or aligners instead of cutting the teeth down?+
We did, in fact, present orthodontics as the first option at consultation. With Invisalign or fixed braces, the supra-erupted central could be intruded back up into the bone, and the palatally tilted central could be torqued labially into line, all without removing any natural tooth structure. That is, in a textbook sense, the most conservative approach to her case.
But the orthodontic option came with three real costs that did not exist with crowns. Time — about 14 to 18 months in appliances for a result this specific. Money — the orthodontic phase alone was quoted at roughly twice the cost of the two crowns. And retention — once the teeth had been moved, both teeth would need a fixed lingual retainer wire bonded for life, because the same forces that allowed them to drift the first time would still be there.
Ms. Ammarah took two weeks to think about it and came back with a clear preference for the crown route. Her stated reason was that she did not want to be in any kind of appliance during the year she was scheduled to be in her brother's wedding photos. That is a reasonable patient-led decision. We documented it, signed it, and moved forward.
Do the teeth underneath the crowns still need root canals?+
No — and we want to be specific about why, because this is a worry we hear at every consultation for anterior crowns.
Root canal treatment is needed when the pulp of a tooth has become irreversibly inflamed or necrotic, almost always because of decay, trauma, or a fracture that has reached the nerve. None of those situations applied to Ms. Ammarah. Both centrals tested vital with a cold stimulus before preparation, and the X-rays showed completely healthy periapical bone with no peri-apical radiolucency.
The amount of tooth structure we remove for a zirconia crown — about 1.0 mm labially and 1.5 mm incisally — is well within the safe envelope for a vital tooth. We use a high-volume water spray during the preparation to keep the pulp temperature from rising, and we cement with a low-thermal-conductivity dual-cure resin cement that the pulp tolerates well. In about 1 in 50 anterior crown cases the pulp can later develop sensitivity that does not resolve, and a root canal is needed retrospectively. For Ms. Ammarah, neither tooth has shown any sign of pulpitis at six months or twelve.
How much did this cost in total? Are there hidden charges over time?+
The two zirconia crowns for Ms. Ammarah, including the consultation, the photographic study, the temporary acrylic crowns, both lab-fitting visits, and the final polish, were quoted at a single all-inclusive fee. No add-ons appeared on the final invoice that were not on the original written quote.
Over time, the only ongoing cost is the six-monthly recall — and the marginal check at that recall is complimentary. A routine scaling at the same visit, if she chooses to add one, is charged separately at our standard scaling fee.
For a comparable case, we generally quote anywhere between PKR 95,000 and PKR 130,000 depending on the laboratory used (we work with one local laboratory and one Pakistan-based zirconia mill), the number of shade try-in visits required, and whether a temporary mock-up is needed before preparation. Every patient receives a written, itemised quote at consultation before any work begins. There are no balance-due surprises later.
The follow-up visits.
A crown is not finished on the day it is cemented — it is finished six months later, after the gum has fully adapted to the new shape and the patient has lived with the new bite long enough to flag anything that does not feel right. Here is how Ms. Ammarah's follow-up cycle went.
Ms. Ammarah came in for a 15-minute review at one week. We checked the bite again with articulating paper, polished a single high spot we found on the upper-right crown, and checked the gum at the cervical margin. No bleeding on probing at either crown. She reported zero sensitivity to hot or cold, which we expected given that the pulps had been protected throughout preparation.
The gum at the cervical margin of both crowns had matured fully — the slight pink halo we sometimes see in the first three weeks after a sub-gingival shoulder had resolved. The interdental papillae were filled, with no black triangle visible between the two new crowns. She had not had to make any adjustments to her chewing habits.
She came back for her complimentary six-month marginal check. We took the same six photographs and compared them side by side with the day-of-cementation set on the screen. No marginal staining, no crown chipping, no occlusal wear on the opposing lower incisors. We took the chance to do a routine scaling of all four quadrants that same visit and booked the twelve-month review.
Twelve months out, the crowns were indistinguishable from the day of cementation. She brought photographs from her brother's wedding — the result she had specifically planned the timeline around — and we filed them alongside the case record. Next recall booked for the six-month mark again, this time complimentary with no scaling required.

Dr. Mian Momin Ahmad
“Cosmetic crown cases like Ms. Ammarah's are about restraint. The temptation in dentistry is always to do more — four veneers instead of two crowns, eight instead of four, a full smile makeover when the patient came in for a single asymmetry. The right plan is almost always the smaller one. Two crowns, on the two teeth that were actually the problem, with the other ten anterior and posterior teeth left untouched. That is the kind of dentistry I want to be doing in twenty years.”
Six small habits that hold the result for two decades.
Anterior crowns last as long as the gum and bone underneath them are kept healthy. These six habits are the only ones we asked Ms. Ammarah to commit to — none of them require buying anything expensive.
Treat zirconia like a natural tooth, not better than one
Zirconia is extremely strong — modern monolithic zirconia survives biting forces that would chip natural enamel. That sometimes leads patients to think they can use it for things they would never do with a natural tooth. They should not. We asked Ms. Ammarah not to bite into apples or chicken bones with her front teeth, not to use them to open packaging, and not to chew ice. The tooth root underneath the crown is still vital natural tooth structure, and the cement layer at the margin is its weakest point.
Floss every night, especially around the new margins
The shoulder margin where the zirconia meets natural tooth structure sits just at the gum line. Plaque that gathers there is the single most common cause of marginal inflammation around a crown. A waxed dental floss, slid carefully through the contact, then drawn gently along the side of the crown, takes about ten seconds per tooth. Done nightly, this single habit is what makes the difference between a crown that lasts 8 years and a crown that lasts 18.
Use a soft brush, not a medium or hard one
Hard bristles can scratch the highly polished labial surface of zirconia over time and, more importantly, will accelerate gum recession at the cervical margin — which would eventually expose the dark line between crown and root. We sized her up for an Oral-B Sensitive head and asked her to brush in small circles, not back-and-forth, at the gum-line for two minutes morning and night.
Come in if the bite ever feels "off"
Zirconia does not wear down at the same rate as enamel. In a person with mild parafunctional grinding, the opposing lower teeth can wear faster than they used to. That can shift the bite over months. The fix is a five-minute occlusal-adjustment appointment with articulating paper — not a re-do of the crown. We asked Ms. Ammarah to flag any new sense of "the teeth meeting wrong" the moment she noticed it, not to wait six months.
Skip whitening on the rest of your teeth — at least for now
Zirconia does not whiten. Once the crowns are made and the shade is matched, any bleaching of the surrounding natural teeth will create a visible shade jump at the canine. We asked Ms. Ammarah to wait at least six months before considering any whitening, and even then to bring in the current shade tab so we could plan it carefully. Most patients in her situation decide they don't need whitening at all once the symmetry is restored.
Six-month recall, every year
Every patient with crowns or bridges at our clinic comes back at six months for a complimentary marginal check. We photograph the cervical margin under magnification, probe the gum at six points around each crown, and remove any plaque that has gathered where her floss could not quite reach. Twenty minutes, no charge for the check, and it catches almost every long-term complication while it is still easy to address.
The longer you wait, the more drift becomes the new shape.
Two teeth that have drifted out of position for a decade do not put themselves back. Every year a supra-erupted tooth stays in supra-eruption, the opposing tooth on the other arch slowly adapts to it — erupting upward, or wearing differently. The lateral incisors begin to compensate. The bite re-balances around the new position. By the time someone in Ms. Ammarah's position has waited an extra five years, the case has stopped being purely about two teeth.
What waiting another five to ten years actually does, in plain terms:
None of that is a scare tactic. It is the pattern we see in our chair. Ms. Ammarah came in when the case was still about two teeth. The fix at this stage was two zirconia crowns and three visits across two weeks. The fix at year ten would have been something larger.
More on crowns and the conditions behind them.
Three more crown and bridge patients.
Every case in this archive is a real Odonto patient with their written consent. Names are accurate where the patient was happy to share them, ages are real, and every photograph was taken in our Engineers Town clinic.


Want a result like Ms. Ammarah's?
The first 15 minutes are free. We will examine your teeth, take any photos needed, and put a written quote in your hand. There is no pressure to book the work the same day, and there are no hidden charges if you do.