A medically complex case, solved with pink-porcelain gingiva — Ms. Khalida's story.
Ms. Khalida is a 57-year-old patient living with hypertension and type-2 diabetes mellitus. She came in with grossly carious anteriors, severe gum recession, and no realistic way to restore the missing vertical height of her smile with conventional crowns alone. This is the case file for the phased PFM rehabilitation — with prosthetic pink-porcelain gingiva built into the bridge — that gave her function and confidence back.
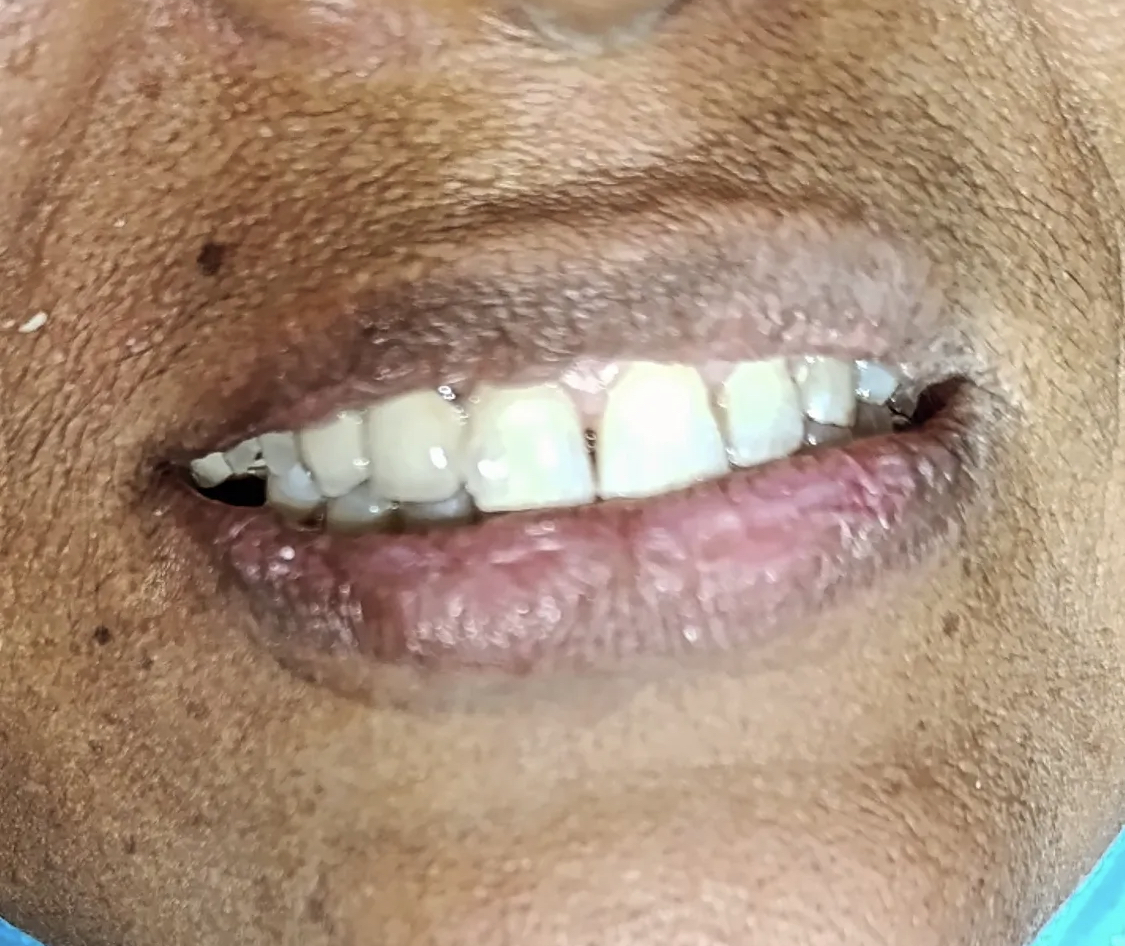
 Before
Before After
AfterA patient with a long medical history. A dental case that needed a different kind of plan.
Most rehabilitation cases at this clinic are predominantly dental problems. Ms. Khalida's case was a medical-plus-dental problem, and the medical side shaped the dental sequencing at every stage.
Ms. Khalida came in to our Engineers Town clinic last winter, accompanied by her son who had driven her from a nearby suburb. She is 57 years old, a homemaker, and a patient with two long-standing systemic conditions: essential hypertension, managed for the past twelve years, and type-2 diabetes mellitus, diagnosed eight years earlier. Both conditions were under the care of her family physician, with reasonable medication adherence and routine quarterly reviews.
Her dental complaint was direct. Her upper front teeth had broken down progressively over the past four or five years. She had stopped chewing on them many months earlier. Smiling in front of family had become uncomfortable. She had been managing with the back teeth and a kind of soft-food diet that her daughter-in-law had quietly built around her constraints. Three months before coming to see us, she had also lost the use of two lower-left posterior molars to severe decay.
The first visit was a full diagnostic appointment. Blood pressure measured (148/92 — slightly elevated but within her usual range), HbA1c reviewed (7.6%, acceptable), medical history documented in full. Then the clinical examination: every tooth charted, every surface checked, every probing depth recorded. Two periapical X-ray sets, one panoramic radiograph. Six intra-oral photographs.
The findings were stark. Four upper anterior teeth grossly carious, broken to the gum on the right and left central incisors, deeply destroyed on both laterals. Two lower-left molars with sub-gingival caries extending below the gum line, non-restorable. Severe gingival recession across the entire upper anterior region, with visible exposure of root surface on multiple teeth. Her bone level — confirmed on the panoramic — was reduced anteriorly but adequate for a fixed bridge approach if abutment teeth were selected carefully.
The aesthetic challenge was significant. Even after extraction of the non-restorable anterior teeth and placement of a fixed bridge across the upper arch, the new teeth would have to be designed in a way that compensated for the missing gum height. A naive approach would have produced unnaturally long teeth. The better answer — and the one we discussed with her over a 45-minute consultation — was to build pink-porcelain prosthetic gingiva into the cervical aspect of the bridge, restoring both the missing tooth crown and the missing gum height in a single seamless restoration.
We obtained written medical clearance from her physician, scheduled the staged extractions a week apart, and started the rehabilitation. She signed the treatment plan after taking it home for three days to discuss with her son and daughter-in-law.
There is a longer story behind why a patient like Ms. Khalida ends up in this state by her late fifties. It is rarely a story of neglect in any straightforward sense. In her case, the slow progression had been the consequence of two parallel factors. The first was that her diabetes had been diagnosed only eight years earlier, after several years of symptomatic but undiagnosed disease. During those undiagnosed years, her salivary glucose levels were higher than they should have been, which silently accelerated the rate of dental caries on her existing teeth. The second was that she had no regular dental check-up routine — visits had been reactive, in response to pain, rather than proactive, looking for trouble before it became symptomatic. The combination meant that decay progressed silently between symptomatic episodes, and by the time any individual tooth started producing acute pain, the underlying caries had usually destroyed enough structure to make conservative restoration impossible.
Knowing this background changed the way we approached the rehabilitation. The technical work was, in its component parts, routine — extractions, fabrication of a transitional appliance, master impression, multi-stage bridge try-in, and final cementation. What was not routine was the way we paced those components. A patient with diabetes needs longer healing periods between surgical phases, more careful tissue management around future bridge margins, and a more intensive home-care regimen during the healing window. Every part of the plan had a slight modification baked in to account for the systemic context, and those modifications were what made the case predictably successful rather than predictably complicated.
The aesthetic problem was, in some ways, the part we were most pleased with how we solved. Severe anterior gingival recession is a difficult finding to manage in any patient, because the missing gum height creates a choice between making the new teeth too long (which looks unnatural) or leaving the cervical zone visible (which exposes root surface that the bridge was never designed to cover). Pink-porcelain prosthetic gingiva, built into the buccal-cervical aspect of the bridge framework, solves the problem by restoring both the missing tooth and the missing gum in a single seamless restoration. The shade of the pink ceramic was matched against the natural gingiva of her lower arch, and the transition zone was almost invisible at conversational distance. For a patient who had stopped smiling in family photographs for years, the visual result was transformative.
The functional result was equally important. Before treatment, Ms. Khalida had not been able to chew on her front teeth for many months — the destruction had left her with no functional anterior occlusion. Her daughter-in-law had quietly built a soft-food diet around her constraints, and the family had stopped suggesting outings that involved restaurant meals. By the four-week mark after final cementation, she was eating on both her front and back teeth comfortably, and the family had marked the occasion by going out to a restaurant for the first time in over a year. The dental work was the immediate clinical intervention; the change in daily life was the actual outcome.

Four findings, each one shaped by her medical history.
In a medically complex patient, every dental finding has to be read against the systemic context that produced it. Ms. Khalida's case is a clear example of how diabetes and dental destruction feed each other over years.
Grossly carious maxillary anterior teeth
Ms. Khalida's upper front teeth were extensively destroyed by long-standing decay. On clinical examination the crowns had broken down to the level of the gum on several teeth, with sharp residual root walls in two places. The destruction was the cumulative result of years of untreated proximal caries — a pattern we see frequently in patients with poorly controlled diabetes, where higher salivary glucose levels accelerate the bacterial acid attack on enamel and dentine. The smile line had collapsed, the lip support had been lost, and chewing on the anterior teeth had become impossible.
Severely compromised posterior molars
In addition to the anterior destruction, two of the lower-left posterior molars were also beyond conservative restoration. The crowns were broken down past the cement-enamel junction with sub-gingival caries extending below the gum line. These teeth had pulpal involvement and very limited remaining tooth structure for any kind of crown to seat onto. They were classified as non-restorable and added to the extraction list.
Severe anterior gingival recession
The chronic plaque retention around the failing anterior teeth had caused the gum to recede significantly in the upper anterior region. By the time we examined her, there was visible exposure of the root surface on multiple teeth and a substantial loss of the vertical height of the gum in the smile zone. Any future prosthesis was going to face an aesthetic challenge — long teeth and short gum, or a much more imaginative solution involving prosthetic pink-porcelain gingiva.
Medically complex — hypertension and diabetes mellitus
Ms. Khalida is a known case of essential hypertension and type-2 diabetes mellitus, both under medical management. Her HbA1c at the time of consultation was 7.6%, which is acceptable for extensive dental work, but it required us to coordinate the case with her physician and modify our protocols — careful pre-operative blood pressure measurement at every visit, antibiotic prophylaxis at extractions, longer healing periods between phases, and a specific written aftercare plan for blood sugar control during the immediate post-operative period.
Four phases. Eleven weeks. Coordinated with her physician throughout.
Every phase was planned with extended healing windows, prophylactic antibiotic cover at extractions, and blood-pressure measurement at the start of every visit.
Medical clearance and phased extractions
Before any irreversible treatment, we corresponded with Ms. Khalida's physician to confirm her hypertension and diabetes were stable enough for staged extractions. With clearance in hand, we extracted the non-restorable upper anteriors and the two compromised lower-left molars in two separate appointments — never both arches in the same week. Each extraction was done under local anaesthesia with antibiotic cover, and we provided sutures and a written 48-hour care sheet at every appointment.
Visits 1-2 · ~ 60 min eachHealing phase and provisional prosthesis
After the extractions, we placed an immediate transitional acrylic partial denture so she would never go without front teeth in public. The healing period was eight weeks — longer than for a non-diabetic patient — to allow full ridge consolidation before any final impression. We reviewed her at weekly intervals during this phase, monitoring tissue healing and blood pressure at every visit.
Weeks 1-8 · transition phaseMaster impression and pink-porcelain wax-up
Once the ridge had healed and the gum architecture had stabilised, we took the master impression for the new PFM bridges. The aesthetic challenge — restoring teeth of the correct length while compensating for the severe gum recession — was solved by designing pink-porcelain prosthetic gingiva into the buccal aspect of the bridges. A diagnostic wax-up was completed in the dental laboratory and shown to Ms. Khalida for approval before the final ceramic work began.
Visit 3 · ~ 50 minPFM bridge try-in, gingival shading, cementation
The new bridges came in two arches. We tried in the metal substructure first to check fit and occlusion, then the biscuit-bake with the pink-porcelain gingiva already shaded to match her natural gum tone, and finally the glazed prostheses just before cementation. The pink porcelain was shade-matched against the natural gingiva of her lower arch under both daylight and clinic light. Final cementation was performed with self-adhesive resin cement.
Visits 4-6 · across 5 weeks During — provisional phase
During — provisional phase During — biscuit-bake try-in
During — biscuit-bake try-inSame patient. A restored smile line and visible lip support.
Drag the divider across the photo to compare. The pink-porcelain gingiva built into the bridge is the difference between a long-toothed prosthesis and a natural-looking result.
BeforeAfterWhy diabetes shapes every dental decision we made.
Three things change in dentistry once a patient has poorly compensated or even well-compensated diabetes. Ms. Khalida's plan reflected all three.
Wound healing is slower in diabetes
Higher blood sugar levels reduce the rate at which extraction sockets close and granulation tissue forms over surgical wounds. For a non-diabetic, an extraction socket is well-healed by week 4. For a diabetic with an HbA1c around 7.5%, the same socket may need 6 to 8 weeks before any prosthetic loading is appropriate. We built that extended healing window into the timeline rather than trying to fit her into a non-diabetic schedule.
Infection risk is higher at surgical sites
Diabetic patients have a small but measurable elevated risk of post-extraction infection — both because of slower healing and because higher salivary glucose feeds a more aggressive bacterial flora. We use prophylactic antibiotic cover at every surgical visit for diabetic patients, and a chlorhexidine mouthwash regimen during healing. This is standard for the literature, not a personal preference.
Plaque control at bridge margins must be obsessive
The single largest contributor to late bridge failure in any patient is plaque accumulation at the cervical margin. In a diabetic patient, the consequences of that plaque arrive faster — gingival inflammation within weeks rather than months, marginal breakdown within a year rather than five. The aftercare regimen we prescribed for Ms. Khalida is therefore more intensive than for a non-diabetic patient of the same age.
Five questions our medically complex patients always ask.
These are the worries we heard from Ms. Khalida and the worries we hear from most patients with hypertension or diabetes considering extensive dental work. Tap any one to read the long answer.
Is it safe to do this much dental work on a diabetic patient?+
Yes — when it is staged correctly and coordinated with the patient's physician. The risks of extensive dental work in a diabetic patient are well understood: slower wound healing, higher post-operative infection rates, and a small risk of intra-operative blood-pressure or blood-sugar destabilisation in patients with poorly controlled disease.
For Ms. Khalida, we addressed each of these in turn. Her HbA1c at consultation was 7.6%, which is within the safe range for elective oral surgery. We obtained written medical clearance from her physician before any extractions. We extended healing periods between phases to twice the duration we would use for a non-diabetic patient. We used prophylactic antibiotic cover at the extraction visits. We measured her blood pressure at the start of every appointment and would have postponed any visit where the systolic exceeded 160.
With those modifications in place, this case is well within the standard of care. Patients with diabetes deserve excellent dentistry, and the answer is never to do nothing — it is to do the right things, in the right order, with the right precautions.
What is the artificial gingiva, exactly? Is it visible?+
Pink-porcelain prosthetic gingiva — sometimes called pink porcelain or pink ceramic — is a specially formulated dental ceramic that imitates the colour and surface texture of natural gum tissue. It is built into the buccal-cervical aspect of the bridge framework, in the area where the patient's own gum has receded.
For Ms. Khalida, the recession in the anterior region was so severe that any bridge designed without prosthetic gingiva would have produced unnaturally long-looking teeth. By incorporating pink ceramic at the cervical margin of the bridge, we restored both the missing tooth structure and the missing gum height at the same time. The shade of the pink ceramic is matched against the patient's own natural gum at biscuit-bake try-in, so the transition from prosthetic to natural gingiva is essentially invisible in normal social distance.
Up close, with strong lighting and the lip retracted, an experienced eye can sometimes detect the transition line. At a normal speaking or photographing distance, it is undetectable.
Could implants have been a better option instead of this bridge?+
For a patient with stable diabetes and no significant smoking history, implants are a legitimate alternative to a fixed bridge. We discussed implants with Ms. Khalida at consultation and walked through the trade-offs honestly.
Implants would have meant: a longer total timeline (typically 4 to 6 months for osseointegration before final loading); a higher overall cost (roughly two to three times the cost of a bridge); a need for at least one surgical procedure with a 4 to 6 month healing window; and a higher risk of late peri-implantitis in a diabetic patient, even with good control.
The bridge option offered a faster timeline (about 11 weeks total), a substantially lower cost, no additional surgery beyond the necessary extractions, and a predictable 12-to-15-year service life with good maintenance. Given her age (57), her medical status, and her stated preference for the most predictable, fastest route to a working smile, the bridge was the right choice for this patient. Implants remain an option for the future if she ever wishes to revisit them.
How long will the artificial gingiva look natural? Does it stain?+
Pink-porcelain prosthetic gingiva is one of the more colour-stable materials in dentistry. It does not absorb dietary pigments the way composite resin does, and it does not fade under UV exposure the way some acrylic gingiva does. With ordinary home care, the pink ceramic will retain its colour for the full lifespan of the bridge — typically 12 to 15 years.
The one thing that can change the visual transition is the gum on the patient's side of the line. If the patient's own gum becomes inflamed and redder than usual, the contrast with the prosthetic gingiva can become briefly visible. Resolving the inflammation — with better home care or a short course of chlorhexidine rinse — restores the invisible transition. We will check this at every six-month recall.
How do I know if my diabetes is well-enough controlled for this kind of work?+
The single most useful number for assessing whether a diabetic patient is ready for elective oral surgery and prosthetic rehabilitation is the HbA1c — a blood test that gives an average of glycaemic control over the previous three months. We obtain this number at the diagnostic visit, either from the patient's recent medical records or from a fresh test if the most recent one is over four months old.
For elective surgical procedures including extractions and minor oral surgery, the published evidence supports a target HbA1c of 8.0% or lower. Below that threshold, wound healing and infection rates are comparable to non-diabetic patients with appropriate antibiotic cover. Above that threshold, healing is meaningfully slower and the risk of post-operative infection rises substantially. Ms. Khalida's HbA1c at consultation was 7.6% — comfortably within the safe range — and we proceeded on that basis.
For non-surgical prosthetic work — bridge preparation, impressions, try-ins, cementation — the HbA1c is less directly relevant. What matters more is the patient's current symptomatic blood-sugar status on the day of the appointment. We always measure blood pressure at the start of every visit, and a diabetic patient who reports feeling unwell on the day of an appointment is rescheduled rather than treated. This is standard care, not over-caution.
What if I lose another tooth later? Will the bridge still work?+
For a patient with multiple medical co-morbidities and significant prior dental history, the realistic possibility is that another tooth may need extraction in the future. The bridge has been deliberately designed in sectional units rather than a single continuous arch, precisely because we wanted to plan for this contingency.
If a future extraction were needed in a sector covered by one of the bridge segments, that single segment can be removed, the extraction performed, and either the segment re-fitted with an additional pontic added, or a new segment fabricated — without disturbing the other sections of the rehabilitation. This kind of sectional planning is standard practice for medically complex patients, and it is the reason a bridge of this size is rarely an “all or nothing” restoration.
We will see Ms. Khalida every six months indefinitely. Any threatening lesion on any remaining natural tooth will be identified and treated at the smallest possible stage. The plan is to delay any further extraction as long as biologically possible.
The follow-up visits.
A full-mouth rehabilitation in a medically complex patient needs a different recall schedule from a routine case. Here is how Ms. Khalida's follow-up cycle has gone.
Routine bite check, marginal probing, and confirmation that healing was on track. She reported full functional comfort and was eating on both sides for the first time in over two years. Blood pressure on the day was 138/86 — improved from the consultation reading.
The natural-gingiva-prosthetic-gingiva transition zone had matured cleanly. No inflammation at any margin. She demonstrated her super-floss technique under the pontics — competent. A short scaling was performed at this visit.
Six-monthly recall with full marginal check, photographic comparison, probing depths and a routine scaling. All margins sealed, all probing depths under 4 mm. Her HbA1c at the same time was 7.1% — improved, and a credit to her own discipline. Next recall booked for the six-month point again.

Dr. Mian Momin Ahmad
“Cases with severe gingival recession used to be treated by accepting unnaturally long teeth in the final prosthesis. Modern pink-porcelain prosthetic gingiva changes that — and for medically compromised patients like Ms. Khalida, where surgical gum grafting is not always advisable, it is the most predictable way to restore the missing vertical height. The case is a reminder that the answer to a difficult problem is often a different design, not a more aggressive surgery.”
Six habits that protect a bridge in a diabetic patient.
Bridge longevity in a diabetic patient depends as much on systemic control as on local hygiene. Both have to be addressed.
Keep your HbA1c under 7.5%
For a patient with diabetes, the single most important determinant of bridge longevity is blood sugar control. Higher HbA1c values mean higher salivary glucose, faster plaque accumulation, and slower healing at every margin. We asked Ms. Khalida to keep her HbA1c at or below 7.5% and to bring her quarterly blood-test results to every six-month dental recall, so we could track the two together.
Brush twice daily with a fluoride toothpaste
Standard fluoride toothpaste, twice a day, with a soft-bristled brush — exactly the same as for any crown or bridge patient. The fluoride matters more for a diabetic patient because the root surfaces of any teeth still in the mouth are particularly vulnerable to acid-induced demineralisation. We sized her up for an Oral-B Sensitive head and a Sensodyne or Colgate Total paste.
Use super-floss under the pontics every night
Like every bridge patient, Ms. Khalida needs to clean under the pontics — the tooth-shaped pieces that bridge the gap between abutments. Super-floss, slid carefully under each pontic once a day, dislodges the plaque that ordinary brushing cannot reach. Done nightly, it is the single habit that will determine whether her bridges last 12 years or 20.
Watch the natural-bridge-natural transition zones
Where the new pink-porcelain gingiva meets her own natural gum at the bridge edge, the tissue can be particularly sensitive in the first few months. We asked her not to use any abrasive whitening toothpaste, and to message us immediately if she ever felt the gum become sore or bleed at those edges. A short course of chlorhexidine rinse can resolve almost any early inflammation if it is caught quickly.
Maintain blood pressure between visits
Most dental procedures we will do for her in the future — even routine cleanings — go more smoothly with stable blood pressure. We asked her to keep her antihypertensive medication regimen exactly as her physician has prescribed it, and to bring a recent home-BP log to every recall. If she is ever on the day of an appointment with a systolic above 160, we postpone and reschedule.
Six-monthly recalls — every six months, not every twelve
For a non-diabetic crown patient, twelve-month recalls can sometimes be acceptable. For a diabetic patient with a full-mouth bridge, six months is the right interval. The marginal check, the gum probing, and the photographic comparison together catch any early issue while it is still easy to address.
Doing nothing is not safer than doing something.
A common assumption among patients with diabetes is that dental work is too risky and that the safer choice is to delay until things are absolutely unavoidable. That logic is inverted. Untreated dental infection raises systemic inflammation, worsens glycaemic control, and accelerates the very systemic complications the patient is trying to avoid. The safer choice is staged, well-coordinated dental rehabilitation while the case is still manageable.
Ms. Khalida came in when the case was still rescue-able with a fixed bridge. The pace of dental destruction in a diabetic patient is faster than in the general population. Earlier intervention is almost always smaller intervention.
More on bridges, diabetes, and recession.
Three more crown and bridge patients.
Every case in this archive is a real Odonto patient with their written consent.


Living with diabetes and putting off dental work?
The first 15 minutes are free. We will examine your teeth, check your blood pressure, and put a written quote and a medical-aware plan in your hand. There is no pressure to commit the same day.