Three nights of unbearable pain, resolved in a single afternoon — Mr. Mubeen's story.
Mr. Mubeen is a 40-year-old patient who came in to our Engineers Town clinic exhausted, having lost three consecutive nights of sleep to severe spontaneous pain in a lower-left posterior tooth. This is the case file for the single-visit root canal that resolved his symptoms the same afternoon — three hours from walking in to walking out, with the tooth saved and the pain completely gone.
 Before
Before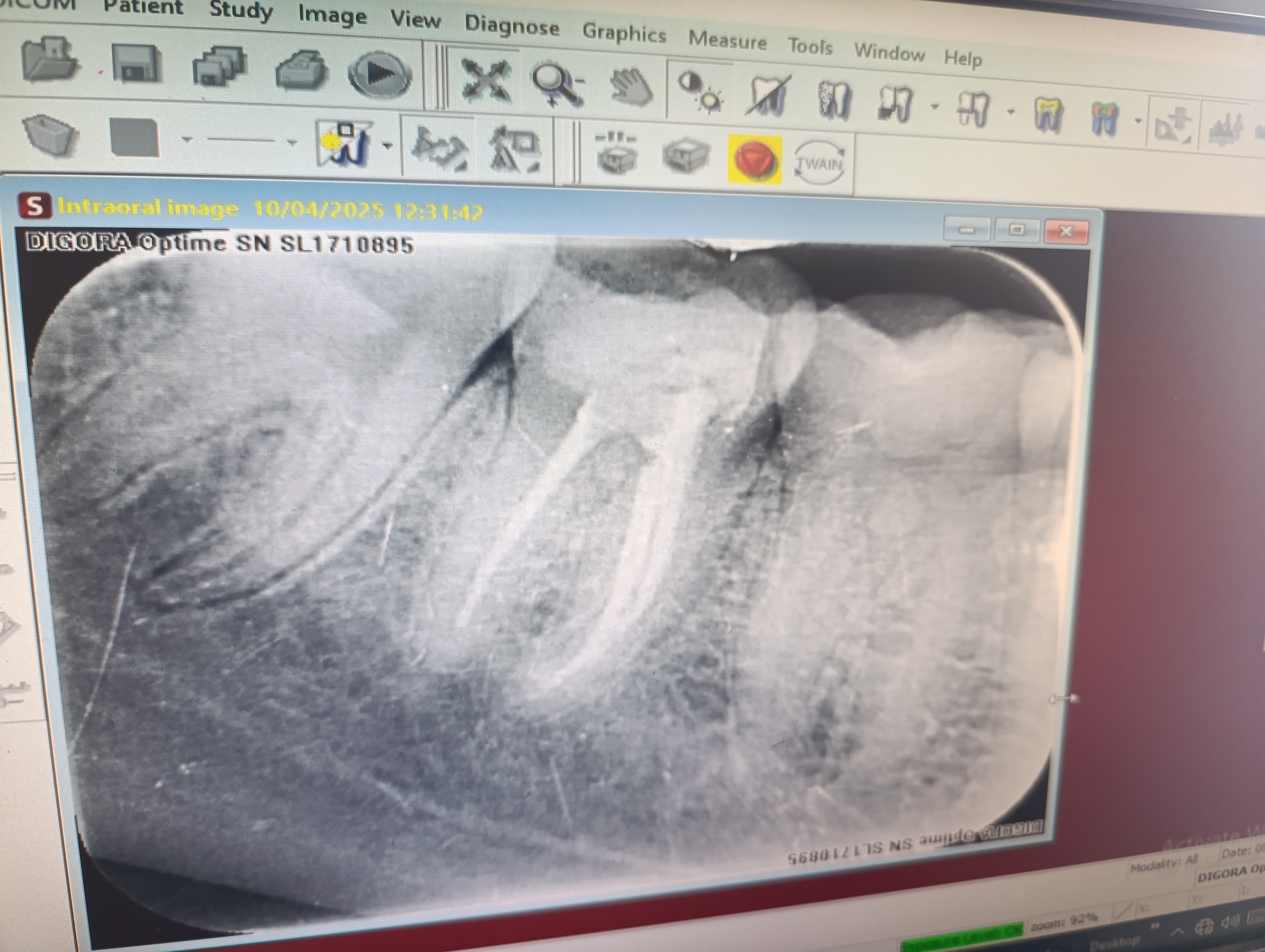 After
AfterThree nights without sleep. One single-visit fix.
Severe night-aggravated tooth pain is one of the most reliable indicators of irreversible pulpitis, and one of the most reliably treatable conditions in adult endodontics.
Mr. Mubeen walked into our clinic on a Tuesday afternoon, in a state of obvious exhaustion. He is 40 years old, working in business administration, and a patient who had spent the previous three nights barely sleeping. The pain in his lower-left posterior tooth had started gradually a week earlier — initially provoked by hot drinks, then by cold ones, and then over the past few days had become entirely spontaneous and worst at night.
He described the pain pattern in detail. It came on without any trigger. It was at its worst when he lay down to sleep, often waking him in the middle of the night with sharp throbbing pain that no over-the-counter analgesic was fully controlling. It was also acutely painful while he was eating — he had stopped chewing on the left side entirely for several days. The pain had begun to dominate his thinking. He had come to the clinic without an appointment, willing to wait, and we saw him within forty minutes.
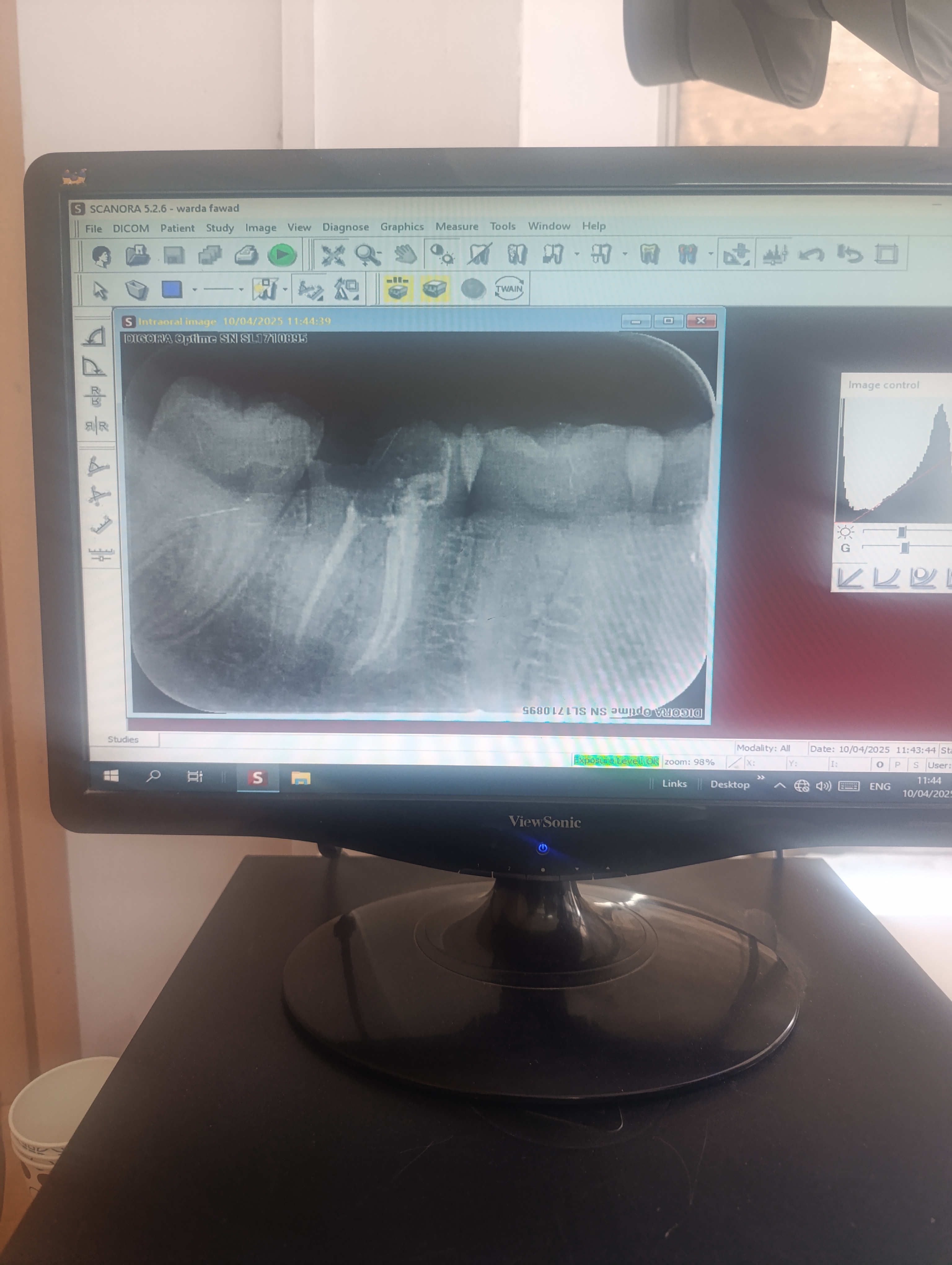
The clinical workup confirmed what the symptom pattern had already suggested. Severe spontaneous pain localised to a single lower-left posterior tooth. A sharp, lingering response to cold testing that persisted for nearly two minutes after stimulus removal. Tenderness on vertical percussion of the affected tooth. Pre-operative peri-apical X-ray showing deep caries with no peri-apical bone changes yet. The diagnosis was symptomatic irreversible pulpitis. The treatment was a root canal.
We had a brief honest conversation about whether to do the procedure the same day or to book it for the next morning after providing emergency pain control. Mr. Mubeen was clear: he wanted it done that afternoon. He had taken half a day off work to come in. He had not slept properly in three nights and wanted to sleep that night. He had no contraindications to extended treatment and no acute abscess that required staged drainage. Single-visit treatment was the right call.
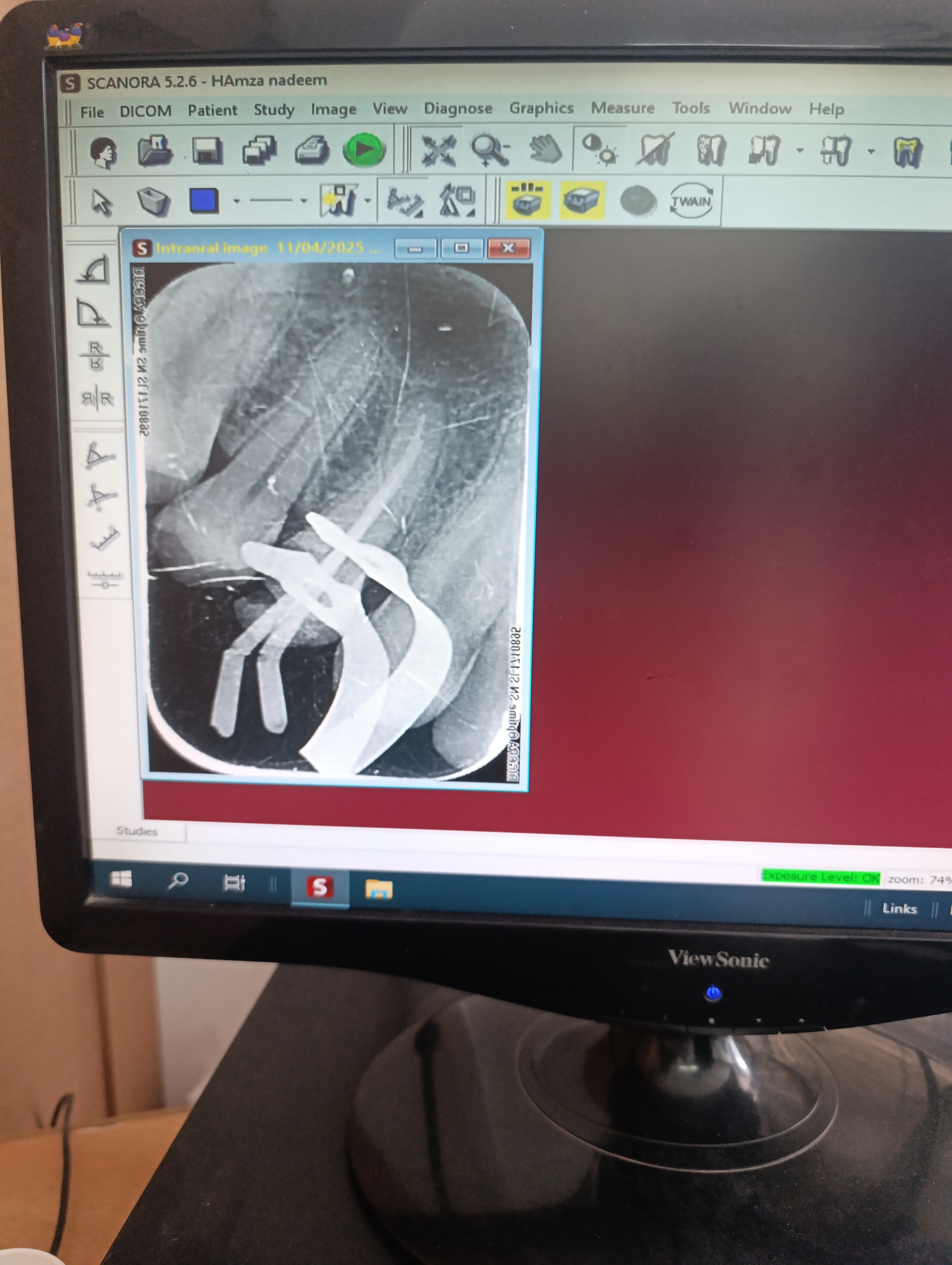
We numbed the quadrant, placed a rubber dam, and performed the root canal in a single session lasting about 2 hours and 45 minutes start to finish. By the time he left the clinic, the tooth was fully cleaned, shaped, dried and obturated. The access cavity was sealed with a composite restoration. The post-operative X-ray confirmed complete fill of all canals. He went home with a written aftercare plan, a five-day course of amoxicillin, a small bottle of ibuprofen for any residual tenderness, and the WhatsApp number to reach us with any question.
He messaged at 11 PM that same evening to confirm he was about to go to sleep — for the first time in three nights — completely pain-free.
The technical details of Mr. Mubeen's case follow a pattern that has become standardised at our clinic for adult single-visit endodontics. The local anaesthesia is established with an inferior alveolar nerve block (for lower-arch cases) using 4% articaine, supplemented with a buccal infiltration to address the soft-tissue innervation of the long buccal nerve. Onset is typically within ten minutes, and the working duration is approximately 90 minutes — enough to complete the entire case in one continuous appointment. The rubber dam is placed over the affected tooth using a Young's frame with a single-tooth clamp. The dam is checked for sealing at the cervical margin and re-positioned if any leakage is detected.
Once the field is dry and isolated, the access cavity is prepared through the occlusal surface using a sequence of high-speed diamond burs followed by a non-end-cutting Endo-Z bur to refine the internal anatomy without risk of perforation. The pulp chamber is irrigated repeatedly with sodium hypochlorite to remove pulp remnants and biofilm. The canal orifices are located visually under operatory magnification — for a posterior tooth this means typically three to four orifices depending on the specific tooth. Size 10 K-files are used to negotiate the apical anatomy before the rotary nickel-titanium instruments are introduced.
The cleaning and shaping phase uses a crown-down sequence — larger files at the coronal end, progressively smaller files at the apical end. The shaping aims to create a continuous taper from the coronal third to the apical third of each canal, which allows the irrigation solutions to reach the apical region effectively and the obturation material to seal the canal three-dimensionally. The working length is confirmed using an electronic apex locator. Once shaping is complete, a final irrigation protocol is performed: 5 ml of sodium hypochlorite, 5 ml of normal saline, 5 ml of 17% EDTA to remove the smear layer, and a final saline rinse. The canals are dried with sterile paper points.
Obturation is performed using a warm vertical compaction technique with gutta-percha and a bioceramic sealer. The bioceramic sealer offers two advantages over older zinc-oxide eugenol sealers: it bonds chemically to dentine through a hydroxyapatite-like reaction at the canal wall, and it is biocompatible enough that any small amount of inadvertent apical extrusion is well-tolerated by the peri-apical tissues. The warm vertical compaction technique uses heated pluggers to plasticise the gutta-percha as it is condensed, which produces a three-dimensional seal that adapts to the canal anatomy at the cellular level.
The access cavity is then sealed with a glass-ionomer base that bonds chemically to the underlying dentine, and a composite resin restoration is placed over the top to restore the occlusal anatomy. A post-obturation peri-apical X-ray is taken to confirm complete fill of all canals to the working length with no voids and no apical extrusion. The bite is checked with articulating paper and balanced if any premature contact is detected. Mr. Mubeen's entire procedure followed this standardised protocol exactly, and the result on the post-obturation X-ray showed a textbook obturation.
Four findings, all consistent with irreversible pulpitis.
The diagnosis was straightforward, the location was specific, and the treatment was clear. Cases like Mr. Mubeen's are why single-visit endodontics exists as a treatment option.
Severe spontaneous pain — disturbing sleep at night
The hallmark of Mr. Mubeen's presentation was the pattern of his pain. It was not provoked by anything — no hot, no cold, no chewing trigger required. It arose spontaneously and was at its worst when he lay down to sleep, often waking him in the middle of the night. This pattern — spontaneous, night-aggravated, no clear stimulus — is one of the most reliable indicators of irreversible pulpitis. The recumbent position increases the intracranial venous pressure slightly, which transmits into the pulpal vasculature, which raises the intra-pulpal pressure, which translates into pain.
Acute, sharp, lingering response to cold testing
When we performed a cold-stimulus test on the affected lower-left posterior tooth, the response was striking — sharp, immediate, and persisted for nearly two full minutes after the stimulus was removed. The two adjacent teeth tested cleanly, confirming the diagnosis was localised to the single offending tooth. A lingering cold response of this magnitude is essentially diagnostic of irreversible pulpitis. The threshold for distinguishing reversible from irreversible pulpitis is typically a response that lasts more than 15 to 20 seconds; Mr. Mubeen's lingered for far longer.
Unbearable pain while eating — the patient had stopped eating on the affected side
In addition to the spontaneous and night-aggravated pain, Mr. Mubeen described an acute sharp pain that occurred while he was chewing. The pain was intense enough that he had completely stopped eating on the left side and had been forcing himself to chew exclusively on the right side for several days. This kind of functional restriction in a 40-year-old man with no other dental issues is itself a strong indicator of the severity of the underlying condition.
Vital tooth — no necrosis yet
Importantly, the cold-stimulus test produced a response — meaning the pulp was still alive, even if catastrophically inflamed. A non-responsive tooth on cold testing would have indicated pulpal necrosis, which is a separate clinical entity with a slightly different treatment approach. The fact that Mr. Mubeen's tooth was still vital meant we were treating the condition before it had progressed to full necrosis — which is the best stage at which to perform root canal therapy.
Four phases. All in one 3-hour single-visit appointment.
The decision to perform single-visit endodontics was made jointly with the patient after a brief honest discussion of the trade-offs. Mr. Mubeen met every clinical criterion for the single-visit approach.
Diagnostic workup and same-day decision
Mr. Mubeen came in to the clinic on a Tuesday afternoon, exhausted from three nights of poor sleep. The clinical and radiographic workup took 25 minutes: cold and percussion tests on the affected tooth and the neighbours, a peri-apical X-ray showing deep caries close to the pulp chamber with no peri-apical bone changes yet, and a confirmation of the irreversible-pulpitis diagnosis. We discussed the option of starting treatment the same day versus splitting it across two appointments. Given that he was already exhausted and the case had no acute abscess, single-visit treatment was the better choice.
Phase 1 · ~ 25 minLocal anaesthesia and access cavity preparation
We administered an inferior alveolar nerve block with 4% articaine and supplemented with a buccal infiltration. Complete anaesthesia of the lower-left quadrant was established within ten minutes. We placed a rubber dam over the affected tooth and prepared the access cavity through the occlusal surface. The pulp chamber was visibly inflamed — consistent with the irreversible-pulpitis diagnosis. We removed the inflamed pulp tissue (pulp extirpation) and irrigated with sodium hypochlorite.
Phase 2 · ~ 35 minWorking length determination and canal preparation
Using a combination of size 10 K-file hand instrumentation and an electronic apex locator, we established the working length for each canal of the lower posterior tooth. Once the working length was confirmed, we cleaned and shaped each canal using a sequence of rotary nickel-titanium files to a standardised final dimension. Sodium hypochlorite irrigation was performed between every pass to dissolve residual pulp tissue and disinfect the canal walls. A final EDTA rinse removed the smear layer.
Phase 3 · ~ 45 minObturation, restoration and same-day discharge
The canals were dried with sterile paper points and obturated with gutta-percha and bioceramic sealer using a warm vertical compaction technique. The access cavity was sealed with a glass-ionomer base and a composite resin restoration. A post-obturation peri-apical X-ray confirmed complete fill to the working length in all canals with no voids. Mr. Mubeen left the clinic with the tooth fully treated, the pain that had been disturbing his sleep completely gone, and a written aftercare plan in his hand.
Phase 4 · ~ 45 minSame tooth. From sleep-disturbing pain to sealed canals — in one afternoon.
Drag the divider to compare the pre-operative X-ray (deep caries with vital but inflamed pulp) with the post-obturation X-ray (canals fully sealed with gutta-percha).
BeforeAfterWhy night-aggravated tooth pain is a textbook signal.
Three biological mechanisms explain why irreversible pulpitis produces a characteristic pattern of severe, spontaneous, night-aggravated pain. Recognising the pattern is half the diagnosis.
The pulp is enclosed in a hard chamber with no room to expand
Most tissues in the body, when inflamed, can swell into the surrounding space — that is what produces the visible swelling around a cut or a bruise. The pulp inside a tooth cannot. It is enclosed in a chamber made of dentine and enamel with only one small exit — the apical foramen at the root tip. When the pulp is inflamed, the increased fluid and white-cell volume has nowhere to go, so the intra-pulpal pressure rises rapidly. The nerve fibres compress under the pressure and signal pain.
Recumbent posture increases the intra-pulpal pressure
When the patient lies down, blood flow gradually redistributes from the legs to the head. The venous pressure in the head increases slightly compared to the standing position. That increase transmits into the pulpal vasculature, which raises the intra-pulpal pressure further, which translates into worse pain. This is why night pain in irreversible pulpitis is often qualitatively worse than the same pain during the day — the patient's own body geometry is amplifying it.
Cognitive distraction during the day masks awareness of constant pain
During the working day, the patient's attention is divided between many inputs — work, conversation, ambient noise, screen time. The brain's constant filter on sensory input reduces the conscious awareness of background pain. At night, in a quiet bedroom with the lights off, the only thing for the brain to attend to is the pain itself. The pain has not actually increased — the perception of it has.
Five questions we hear at every single-visit root canal consult.
These are the worries we heard from Mr. Mubeen and the worries we hear from most adult patients facing a same-day root canal. Tap any one to read the long answer.
Is it really possible to do a complete root canal in one visit?+
Yes — and the published evidence shows essentially equivalent success rates for single-visit and two-visit endodontics in cases without acute peri-apical infection. The difference is not in the biological success but in the clinical workflow.
A single-visit root canal requires the patient to be tolerant of a longer single appointment (typically 90 minutes to 2 hours for a posterior tooth) and requires the case to have no acute fluctuant swelling or draining sinus. For a healthy adult patient with irreversible pulpitis but no abscess — which describes Mr. Mubeen's case precisely — single-visit treatment is appropriate and often preferred.
The technical core of a successful root canal is complete cleaning and shaping of the canal system combined with sodium hypochlorite irrigation. Both happen in the same single appointment in a single-visit case, with the same thoroughness as a two-visit case. The obturation is done while the canals are at their cleanest. The success rate of single-visit endodontics on a vital pulp is between 90 and 95 percent at five years.
Why was the pain worse at night?+
Night-aggravated tooth pain is a classic and reliable feature of irreversible pulpitis. There are two main reasons.
First, when the patient lies down, the intracranial venous pressure rises slightly due to gravitational redistribution of blood flow. That increased pressure transmits into the pulpal vasculature, which is enclosed in a hard chamber with no room to expand. The result is a small but real increase in intra-pulpal pressure, which translates directly into worsening pain on the inflamed pulp.
Second, the cognitive distractions of the day — work, conversation, ambient noise — partially mask awareness of constant pain. At night, in a quiet bedroom, with no other input to compete with, the pain becomes the dominant sensory experience and feels qualitatively worse. The pain has not actually increased — but the perception of it has.
For Mr. Mubeen, the combination of both factors had been disturbing his sleep for three consecutive nights before he came in. After the root canal, the spontaneous pain resolved completely within hours and he slept normally that same night.
How quickly does the pain resolve after a root canal?+
In most cases of irreversible pulpitis, the spontaneous pain resolves immediately or within hours of the procedure being completed. This is because the source of the pain — the inflamed pulp tissue under pressure in a confined chamber — has been physically removed during the procedure. There is nothing left to produce the pain signal.
Some patients experience a mild residual tenderness on biting for the first 24 to 72 hours, which is the result of the peri-apical bone responding to the disturbance of instrumentation. This tenderness is generally well-controlled with over-the-counter ibuprofen and resolves on its own within three to five days. For Mr. Mubeen, the spontaneous pain that had been disturbing his sleep resolved within four hours of leaving the clinic, and he had no significant residual tenderness even at the one-week review.
Why do I need a crown? Can I just have the composite filling?+
For a heavily loaded lower posterior tooth like Mr. Mubeen's, the published evidence is unambiguous: a crown placed after the root canal substantially extends the long-term service life of the tooth and reduces the risk of vertical fracture under chewing load.
The reason is biomechanical. A non-vital tooth loses some of its internal hydration over years, and the dentine becomes slightly more brittle. Combined with the loss of structural integrity from the access cavity preparation, the cusps become more vulnerable to fracture. A crown encloses the cusps in a single rigid shell that distributes chewing forces across the entire occlusal surface and prevents the wedge-type forces that can split a tooth vertically.
For an upper premolar — like Mr. Aun's case earlier in this archive — the chewing forces are lower and a composite restoration can sometimes be adequate. For a lower posterior tooth in a 40-year-old patient with many decades of chewing ahead, a crown is the right protective measure. The published 10-year survival rate for root-canal-treated lower molars with crowns is around 90 percent; without crowns, it drops below 50 percent.
How do I know if I'm a good candidate for single-visit endodontics?+
Single-visit endodontics is appropriate for a specific clinical profile, and it is part of the clinician's responsibility to identify whether each particular case fits. Three conditions determine candidacy.
The first condition is the absence of acute peri-apical infection. A tooth that presents with frank pus, fluctuant facial swelling, or a draining sinus is not a good candidate for single-visit completion — that kind of case benefits from staged treatment with intracanal medication between visits to allow the acute inflammation to resolve. A tooth with severe irreversible pulpitis but no abscess formation, like Mr. Mubeen's, is an excellent candidate for single-visit treatment.
The second condition is the patient's tolerance for an extended single appointment. A molar root canal in a single visit is a 2-to-3-hour appointment with continuous local anaesthesia and continuous rubber-dam isolation. Some patients prefer this — they would rather finish the case in one sitting and avoid the return visit. Others prefer two shorter visits. Both are valid preferences, and the clinician should ask explicitly which the patient would prefer before proceeding.
The third condition is that the patient is medically stable for the extended appointment. Patients with significant cardiovascular disease, severe anxiety, or other conditions that make a long single appointment uncomfortable are usually better served by a two-visit protocol with shorter sessions. Mr. Mubeen had no such complicating factors, and he was eager to complete the case in one sitting.
For the right patient with the right clinical presentation, single-visit endodontics offers the same biological success rate as two-visit treatment, with the practical advantage of completing the case in one appointment. For other patients, the two-visit protocol is the right choice. The decision should always be based on the specific clinical situation and the specific patient's preferences, not on a clinic-wide default.
What does a single-visit root canal cost compared to a two-visit one?+
At our clinic, single-visit and two-visit root canals on the same tooth are quoted at the same fee — because the technical work is the same. The fee covers the diagnostic radiographs, the local anaesthesia, the rubber-dam isolation, the full endodontic instrumentation, the irrigation, the obturation, and the post-endodontic composite restoration. The single-visit option simply completes that work in one longer appointment rather than splitting it into two shorter ones.
The recommended crown is quoted and billed separately at the crown appointment.
For Mr. Mubeen, the single-visit root canal was completed within a single all-inclusive fee. No additional charges were added at any stage of the appointment.
The follow-up visits.
A single-visit root canal is followed by a one-week restoration review, a crown placement at 6 to 8 weeks, and a peri-apical X-ray review at six months. Here is how Mr. Mubeen's follow-up went.
Mr. Mubeen messaged on WhatsApp at 11 PM that evening — completely pain-free for the first time in three nights. He had eaten dinner on the opposite side and was about to go to sleep.
A short 10-minute visit to check the composite access restoration, percussion-test the tooth, and palpate the gum over the root. All tests clean. The bite was settled. He had completed the antibiotic course and was no longer taking any analgesics.
Tooth preparation, digital scan, and a chair-side acrylic temporary crown were completed at this visit. The final zirconia crown was cemented two weeks later, with the bite balanced and the shade matched to the adjacent lower molars.
A fresh peri-apical X-ray confirmed full peri-apical bone integrity. No widening of the periodontal ligament space. The crown was sealed and functioning normally. He was eating on both sides without any awareness of the treated tooth.

Dr. Mian Momin Ahmad
“A 40-year-old patient who has lost three nights of sleep to severe spontaneous tooth pain is the textbook scenario for single-visit endodontics. The case is well-defined, the diagnosis is clear, the patient is motivated to finish the procedure in one sitting, and the biology of the case is favourable. When we do this well, the patient sleeps through the night the same evening. It is one of the most consequential interventions in general practice.”
Six habits that protect a single-visit root canal.
The aftercare for a single-visit case is essentially identical to that for a two-visit case. The main additional emphasis is the recommendation for a protective crown on a heavily-loaded lower posterior tooth.
Avoid chewing on the treated side for two weeks
A root-canal-treated lower molar is functionally weaker than a vital molar for the first two weeks. Mr. Mubeen was asked to chew on the opposite side for 14 days and to favour the opposite side for soft foods for another month after that.
Plan for a crown within 6 to 8 weeks
For a 40-year-old patient with a heavily loaded lower posterior tooth, a crown is strongly recommended within 6 to 8 weeks of completing the root canal. The crown distributes chewing forces across the cusps and prevents the slow vertical fracture that can develop in a non-vital posterior tooth under prolonged loading. Mr. Mubeen's crown appointment was scheduled at the end of the root canal visit.
Take the prescribed antibiotic course as directed
A five-day course of amoxicillin was prescribed to address any residual peri-apical bacterial involvement. We asked him to complete the full course even if symptoms resolved earlier, which they did within 24 hours.
Brush gently around the treated tooth for the first week
The gum overlying the root of the treated tooth is recovering from a period of inflammation and is mildly tender for 7 to 10 days. A soft-bristled brush, used with light pressure, prevents the gum from being further irritated.
Watch for any return of tenderness or new symptoms
Properly performed root canals almost always heal without complication. In a small minority of cases, a residual infection can persist and produce a recurrence of tenderness, a small lump on the gum, or a sensation of the tooth being slightly “raised”. We asked Mr. Mubeen to flag any return of symptoms on WhatsApp immediately.
Return for the six-month X-ray review
Every root canal patient comes back at six months for a peri-apical X-ray to confirm full bone healing around the root tips. The image is compared against the post-operative X-ray taken on the day of treatment. The review is complimentary at our clinic.
Spontaneous night pain in a tooth does not resolve on its own.
Unlike a dull discomfort or a tooth that feels “sensitive”, spontaneous night-aggravated pain is a sign of irreversible damage to the dental pulp. The condition does not heal without intervention, and waiting another week typically just adds another week of poor sleep without changing the treatment plan. Coming in the same day the spontaneous pain begins is the right thing to do.
Mr. Mubeen came in at day three — the right time. The case was a single-visit root canal completed the same afternoon. Earlier intervention is almost always simpler intervention.
More on root canals and dental emergencies.
More root canal cases.

A tooth keeping you awake at night? Call us today.
We keep emergency slots for severe pain every day. Single-visit root canals are available when the case fits. The first visit will diagnose, give you pain relief, and either start the definitive treatment the same day or book it for the next morning. No pressure to commit without a written quote.